Nandrolone is an anabolic that has earned a reputation for helping athletes feel better while training through tendon and joint pain. That is the reason I was interested in it for climbing: not because climbers need more muscle, but because connective tissue is one of the limiting factors in hard climbing and injury recovery.
The obvious upside is collagen synthesis. In the research I found, nandrolone appears to be one of the more interesting compounds for increasing collagen deposition. For climbers, that sounds attractive on paper. We care about fingers, elbows, shoulders, knees, and the connective tissue that lets us apply force repeatedly without falling apart.
The problem is that more collagen is not automatically better collagen. Tendons need organization, remodeling, and load-specific adaptation. A compound that increases deposition can still create tissue that is stiffer, less organized, or poorly matched to the actual stress of climbing.
This is where 19-nor derivatives get complicated. They can affect sympathetic drive, mood, resting heart rate, estrogen, and prolactin. While using nandrolone, some people report anxiety or depression. In my own testing, I did not experience either, but I did notice my resting heart rate running about 7 to 9 beats per minute higher than usual.
There is also the body-weight problem. Nandrolone is a strong anabolic and can be excellent for bodybuilders trying to add size. That same effect is not automatically useful for climbers. More muscle and more water retention can push body weight up without an equal increase in climbing-specific strength.
Researchers have looked at nandrolone as a possible healing agent in comparison with growth hormone. One Turkish study from 2003 compared recombinant human growth hormone and nandrolone phenylpropionate in healing ischemic colon anastomosis in rats. Collagen deposition increased in both groups, but the therapeutic effects were more favorable in the growth hormone group.
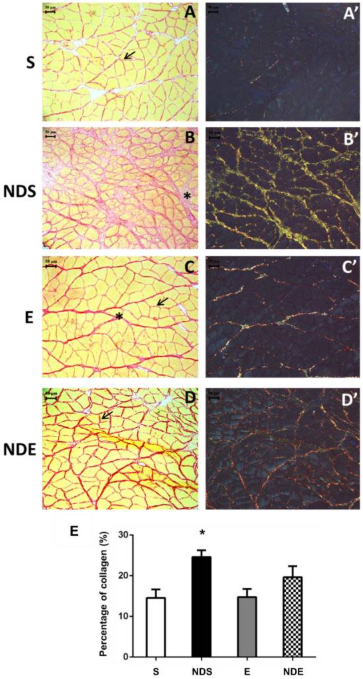
Another study, Effects of Nandrolone Decanoate on Skeletal Muscle and Neuromuscular Junction of Sedentary and Exercised Rats, gave rats a very high nandrolone dose and compared sedentary and exercised groups. The sedentary drug group had the worst-looking tendons, with too much and poorly organized collagen. Exercise improved the picture, but the exercise-plus-drug group still showed disorganized tendon structure compared with exercise alone.
I plan to consult with more tendon experts going forward, but in my last conversation with a couple of doctors, tendons are strongest when collagen depositions are lateral. Vertical collagen depositions may contribute to stiffness associated with anabolic abuse. Bodybuilders often tolerate this because they train for very different loading patterns, but climbers need finger and tendon integrity at a much lower body weight.
There is also an in vitro study where nandrolone was used to stimulate connective tissue growth. In that model, nandrolone decanoate and load acted synergistically to increase matrix remodeling and biomechanical properties of bioartificial tendons.
My takeaway is that load matters. If a tendon is not being trained, simply adding a compound that increases collagen deposition can produce tissue that looks worse. If a tendon is being loaded intelligently, nandrolone may improve the amount of remodeling and strength, but the result may still be suboptimal for climbing compared with other approaches.
My personal conclusion is that nandrolone has a place in enhancing collagen synthesis, but I do not think it is ideal for rock climbers. The water gain, muscle gain, heart-rate change, hormone-management complexity, and possibility of disorganized tendon remodeling make it too blunt for the sport. If I were a grip athlete in an open division, I would think about it differently. For climbing, I would rather look at approaches that improve tendon integrity without the same tradeoffs.
Think I am wrong? Email anabolicclimbing@gmail.com, and if I am, I will post a correction.